Learninsta presents the core concepts of Microbiology with high-quality research papers and topical review articles.
Medical Bacteriology of Staphylococcus aureus
The genus Staphylococcus is included in the family Micrococcaceae. Staphylococcus is a normal flora of skin and mucous membranes, but it accounts for human infections, which is known as staph infection.
The name Staphylococcus was derived from a Greek word, ‘staphyle’ means bunch of grapes and ‘kokkos’ means berry. Staphylococcus aureus is a pathogenic species that causes pyogenic infections in human.
Morphology
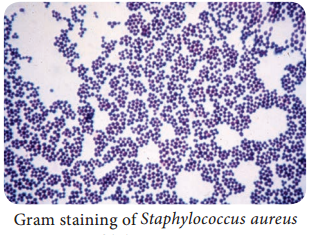
- Staphylococci are gram positive spherical cocci, (0.8µm-1.0µm in diameter) arranged characteristically in grape like clusters (Figure 7.1).
- They are non-motile and non-sporing and few strains are capsulated.
Cultural Characteristics
- They are aerobes and facultative anaerobes, optimal temperature is 37°C and optimum pH is 7.4-7.6.
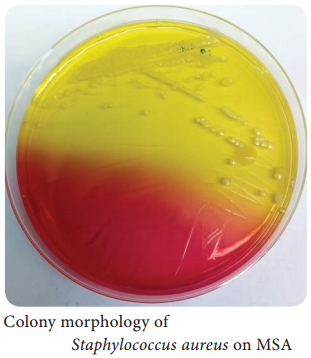
- They grow on the following media and shows the characteristic colony morphology (Table 7.1 & Figure 7.2).
Staphylococci aureus colony morphology on various media
| Media | Colony Morphology |
| Nutrient Agar | Colonies are circular, smooth, convex, opaque and produces golden yellow pigment (most strains). |
| Blood Agar | Beta haemolysis |
| Mannitol salt Agar (MSA) | It is a selective medium for S. aureus produces yellow colored colonies due to fermentation of mannitol. |
Virulence Factors
- Peptidoglycan → It is a polysaccharide polymer. It activates complement and induces the release of inflammatory cytokines.
- Teichoic acid → it facilitates adhesion of cocci to the host cell surface.
- Protein A → It is chemotactic, antiphagocytic, anticomplementary and induce platelet injury.
4. Toxins:
- Hemolysins – It is an exotoxin, those lysis red blood cells. They are of four types namely α-lysin, β-lysin, γ-lysin and delta lysin.
- Leucocidin – It damages PMNL (polymorphonuclear leucocytes) and macrophages.
- Enterotoxin – It is responsible for manifestations of Staphylococcus food poisoning.
- Exfoliative toxin – This toxin causes epidermal splitting resulting in blistering diseases.
- Toxic shock syndrome toxin – TSST is responsible for toxic shock syndrome.
5. Enzymes:
S. aureus produces several enzymes, which are related to virulence of the bacteria.
- Coagulase – It clots human plasma and converts fibrinogen into fibrin.
- Staphylokinase – It has fibrinolytic activity.
- Hyaluronidase – It hydrolyzes hyaluronic acid of connective tissue, thus facilitates the spread of the pathogens to adjacent cells.
- Other enzymes – S. aureus also produces lipase, nucleases and proteases.
Pathogenicity
S. aureus is an opportunistic pathogen which causes infection most commonly at sites of lowered host resistance. (Example: damaged skin) Mode of Transmission: Staphylococcus infections are transmitted by the following ways.
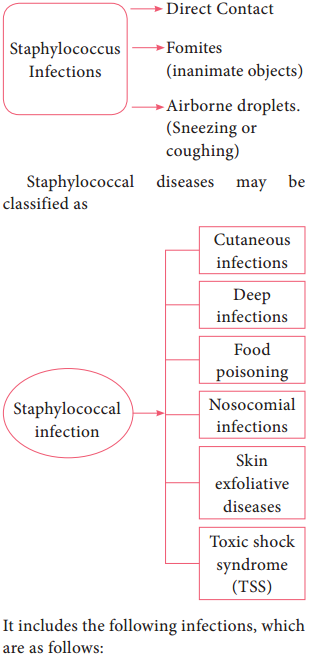
It includes the following infections, which are as follows:
Cutaneous infections:
Wound (injury), burn infections (tissue injury caused by heat), pustules (A small elevated skin lesions containing pus), furuncles (boil forms around a hair follicle and containspus), styes (a painful swelling of hair follicle at eyelids), carbuncles (painful cluster of boils of the skin), Impetigo (skin infection with vesicles, pustules which ruptures), pemphigus neonatorum (an auto immune diseases that affect skin and
mucous membranes)
Deep infections:
It includes Osteomyelitis (inflammation of bones), tonsillitis (inflammation of tonsils), pharyngitis (inflammation of pharynx) sinusitis (inflammation of sinuses), periostitis (inflammation of membrane covering bones), bronchopneumonia (inflammation of lungs), empyema (collection of pus in the body cavity), septicemia (blood poisoning caused by bacteria and its toxins), meningitis (inflammation of meninge), endocarditis (inflammation of endocardium), breast and renal abscess.
Food Poisoning:
Staphylococcal food poisoning may follow 2-6 hours after the ingestion of contaminated food (preformed enterotoxin). It leads to nausea, vomiting and diarrhea.
Nosocomial infection:
S. aureus is a leading cause of hospital acquired infections. It is the primary cause of lower respiratory tract (LRT) infections and surgical site infections and the second leading cause of nosocomial bacteremia, pneumonia, and Cardiovascular infections.
Exfoliative diseases:
These diseases are produced due to the production of epidermolytic toxin. The toxin separates the outer layer of epidermis from the underlying tissues leading to blistering disease. The most dramatic manifestation of this toxin is scalded skin syndrome. The patient develops painful rash which slough off and skin surface resembles scalding.
Laboratory Diagnosis
Specimens:
The clinical specimens are collected according to the nature of Staphylococcal infections, which is given in the (Table 7.2).
Table 7.2: Clinical specimen collected for Staphylococcal infections
|
Infections |
Clinical Specimens |
| Supportive lesions | Pus |
| Respiratory infections | Sputum |
| Septicemia | Blood |
| Meningitis | CSF |
| Food poisoining | Faeces, food or vomitus |
Specimens should be transported immediately to the laboratory and processed.
Direct Microscopy:
Gram stained smears of clinical specimens is done, where gram positive cocci in clusters were observed.
Culture:
The collected specimen is inoculated on selective media-MSA and the media incubated at 37°C for 18-24 hours. Next day culture plates are examined for bacterial colonies, which are identified by gram staining, colony morphology and biochemical tests such as
a. Catalase test:
The genusStaphylococci are catalase positive. This test distinguishes Staphylococcus from Streptococcus (catalase negative).
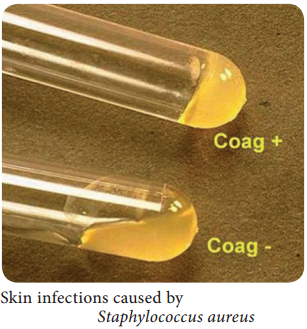
b. Coagulase test:
This test helps in differentiating a pathogenic strain from non-pathogenic strain. S. aureus is coagulasepositive (Figure 7.3).
Treatment
Benzyl penicillin is the most effective antibiotic. Cloxacillin is used against beta lactamase. Producing strains (β-lactamase is produced by few strains of S. aureus which cleaves β-lactam ring of penicillin). Vancomycin is used against MRSA (Methicillin Resistant Staphylococcus aureus) strains.
Topical applications:
For mild superficial lesions, topical applications of bacitracin or chlorhexidine is recommended.
Control measures:
Proper sterilization of medical instruments must be done. Intake of antibiotics must be taken under proper medical advice. The detection of source & carriers among hospital staff, their isolation and treatment should be practiced.